UK’s HEALing Communities Study Begins WAVE 2 Intervention
The University of Kentucky’s $87 million HEALing Communities Study (HCS) to address the opioid epidemic in Kentucky is expanding to more communities across the Commonwealth.
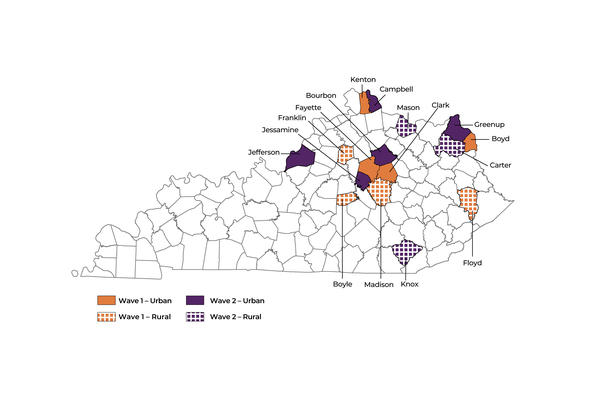
The second wave of the study, known as WAVE 2, was launched in Bourbon, Campbell, Carter, Greenup, Jefferson, Jessamine, Knox and Mason counties July 1. Through the HCS intervention, communities will implement new recovery, treatment and prevention strategies proven to reduce opioid overdose deaths.
Launched in 2019, the ambitious four-year study includes a multidisciplinary team of more than 25 UK researchers and leverages existing resources and initiatives in partnership with communities to implement various strategies to reduce opioid deaths across Kentucky.
The randomized study includes 16 Kentucky counties impacted by opioid abuse and is broken down into two waves of eight counties each. WAVE 1, which includes Boyd, Boyle, Clark, Fayette, Floyd, Franklin, Kenton and Madison counties, was launched in 2020.
Evidence-based practices implemented by the HCS team in partnership with community and state behavioral/health and criminal justice agencies include delivery of medication for opioid use disorder (MOUD), overdose prevention education, distribution of naloxone, a lifesaving medication that reverses the effects of opioids, and reducing risky prescribing.
“Through WAVE 2 the HEALing Communities Study will bring life-changing outreach and access to treatment to thousands of Kentuckians,” said HCS principal investigator Sharon Walsh, Ph.D., a professor in UK’s College of Medicine and College of Pharmacy and director for the Center on Drug and Alcohol Research. “The intervention will also help us better understand what’s needed in each community and where to focus and ramp up efforts to best support individuals to reduce opioid overdose deaths. What we learn will create sustainable solutions for the opioid epidemic in Kentucky that can also be replicated in communities throughout the nation.”
In 2021, overdose deaths reached an all-time high in Kentucky and the U.S., with the Centers for Disease Control and Prevention reporting 107,000 deaths nationally, with a record 2,250 in Kentucky. The HCS team has been adjusting intervention strategies to address the rapidly evolving opioid crisis, including increasing naloxone distribution and expanding outreach and services in communities of color.
In the months prior to the launch of each wave, the HCS team worked with community partners to establish the infrastructure needed to support the intervention. Community coalitions were identified in each county to help guide the intervention and determine what strategies to implement based on individual community needs.
The WAVE 2 intervention includes community engagement to assist key stakeholders in applying evidence-based practices and a communications campaign to build demand for treatment and reduce stigma toward people with opioid use disorder. The HCS team is also working with various pharmacies and health care providers to implement safer opioid prescribing and dispensing.
A recent update shows the impact such strategies have had in WAVE 1 communities since the intervention was launched in 2020. WAVE 1 is now in a sustainability phase, which is intended to build capacity to help community coalitions and partner organizations sustain the evidence-based practices after the study ends.
HCS researchers will now begin to analyze data from WAVE 1 and 2 communities over the past year, using pre-intervention usual care in WAVE 2 as a control. The comparison will show how evidence-based practices work within different settings in each community. The WAVE 2 intervention is expected to end in early 2024.
Research reported in this publication was supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number UM1DA049406. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.

